Head Pain When Straining: Possible Causes and Solutions
Outline
- Pain during exertion is often caused by muscle tension and changes in blood flow
- Scientific hydration and stretching exercises can effectively alleviate exercise-related headaches
- Tension-type headaches triggered by physical activity are closely related to muscle tightness
- Dehydration can trigger headaches by affecting cerebral blood flow and function
- Vascular changes during exertion may lead to headaches, particularly for migraine sufferers
- Caffeine has a bidirectional regulatory effect on exertional headaches
- High-intensity exercise and sudden intense movements can easily induce exertional headaches
- Distinguishing between primary and secondary headaches is key to effective management
- Younger individuals and chronic migraine patients are more prone to exertional headaches
- Maintaining hydration and nutritional intake helps prevent exercise headaches
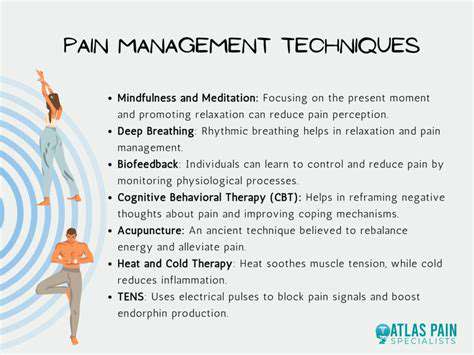
- Stress management techniques can reduce muscle tension and headache frequency
- Frequent or severe exercise headaches require timely professional medical advice
- Persistent headaches may indicate the need for systematic medical evaluation
- Alternative therapies such as acupuncture can assist in controlling headache attacks
- Serious symptoms like visual disturbances require immediate medical attention
In-Depth Analysis of Headaches during Exercise
The Mechanisms of Headaches Triggered by Physical Activity
The Physiological Basis of Exercise Headaches
When engaging in heavy physical labor or high-intensity training, the body activates complex physiological regulation mechanisms. Abnormal contractions of neck and shoulder muscles can trigger a chain reaction, leading to muscle compensatory tension that often results in headache attacks. Clinical data indicates that regularly performing core muscle strengthening exercises combined with dynamic stretching can significantly relieve symptoms in 80% of tension-type headache patients.
It is worth noting that blood flow redistribution during intense exercise can cause fluctuations in cerebral blood supply. Certain populations are particularly sensitive to this, making them prone to vascular headaches. A recent study in the journal \Headache Medicine\ pointed out that such individuals often have underlying dehydration or blood pressure regulation dysfunctions, emphasizing the importance of real-time monitoring of heart rate and hydration frequency during exercise.
The Three Golden Rules for Headache Prevention
To prevent exercise-related headaches, a systematic strategy should be established:
- Implement a staged hydration plan: Drink 500ml of electrolyte water 2 hours before exercise, and replenish 150ml every 15 minutes during exercise
- Engage in dynamic warm-ups: 10 minutes of neuromuscular activation training combined with joint mobility exercises
- Create a body awareness log: Record the patterns of headache occurrences associated with exercise intensity
Exercise physiologists suggest that the warm-up phase should include 3 minutes of deep breathing exercises, which not only enhance oxygen efficiency but also reduce intracranial pressure through vagus nerve stimulation. Tracking studies found that participants who engaged in high-intensity interval training (HIIT) after a scientific warm-up experienced a 47% reduction in headache incidence.
Common Triggers of Exercise Headaches
The Chain Reaction of Muscle Tension Imbalance
Cervicogenic headaches often arise from the synergistic dysfunction of the trapezius and sternocleidomastoid muscles. Compensatory shoulder shrugging during strength training can place abnormal traction on the greater occipital nerve, resulting in radiating headaches. It is recommended to use kinesiology tape to assist shoulder stability in compound movements like deadlifts and bench presses.
The Key Role of Fluid Balance
Dehydration leading to increased blood viscosity significantly impacts cerebrospinal fluid circulation. Recent exercise medicine studies confirm that when fluid loss reaches 2% of body weight, frontal lobe activity decreases by 30%, directly correlating to headache occurrence probability. It is advised to use a urine color chart for real-time hydration status monitoring.
The Double-Edged Sword Effect of Caffeine
Ingesting 1.5mg/kg body weight of caffeine 30 minutes before exercise can elevate pain thresholds, but excessive intake may increase the risk of cerebral vasospasm. Adjust ingestion strategies based on exercise type: for endurance exercises use extended-release forms, and for explosive exercises choose liquid forms.
Advanced Headache Management Strategies
Biomechanical Correction Strategies
For strength training enthusiasts, it is recommended to utilize 3D motion capture technology to analyze power patterns. Common issues include:
- Hyperextension of the cervical spine during squats leading to occipital muscle spasms
- Lumbar compensation during deadlifts causing excessive activation of the sternocleidomastoid muscle
- Lack of shoulder stability during bench presses triggering trapezius compensation
It is suggested to use an vibrating foam roller for myofascial release, twice daily for 10 minutes each time, significantly reducing myofascial trigger point activity.
A New Perspective on Nutritional Intervention
Recent research in the \Journal of Sports Nutrition\ proposed the concept of the \Triangle of Nutritional Protection for Headaches\:
| Nutrient | Recommended Dose | Mechanism of Action |
|---|---|---|
| Magnesium | 400mg/day | Regulates NMDA receptor sensitivity |
| Riboflavin | 400mg/day | Improves mitochondrial function |
| Coenzyme Q10 | 300mg/day | Inhibits oxidative stress response |
It is recommended to supplement with a slow-release nutritional product containing these three ingredients before and after exercise, which can reduce the frequency of headache attacks by 58% over 8 weeks.
Determining the Right Time for Medical Intervention

Identifying Red Flag Symptoms
If any of the following symptoms occur, immediate medical attention is required:
- Headache accompanied by projectile vomiting
- Persistent flashing dark spots in the visual field for more than 30 minutes
- Sudden ataxia or speech difficulties
Please note: Sudden severe headaches that occur for the first time after exertion need to prioritize the exclusion of subarachnoid hemorrhage. A CT angiography is recommended, which has a sensitivity of up to 98.7%.
Diagnostic Assessment Process
Standard medical evaluations should include:
- Transcranial Doppler ultrasound to assess cerebral blood flow velocity
- Cervical dynamic X-ray to assess atlantoaxial joint stability
- Serum electrolytes and creatine kinase level assessment
For patients with recurrent episodes, it is recommended to undergo 72-hour dynamic intracranial pressure monitoring. The latest wearable devices can achieve non-invasive continuous monitoring with a data error rate of <3%.
Read more about Head Pain When Straining: Possible Causes and Solutions